Overview and Pathophysiology
The lifetime prevalence of low back pain is reportedly as high as 84% and is the most common reason adults in the United States use complementary and alternative medicine.
Acute LBP is defined as pain in the lumbosacral region, which has been present for less than 6 weeks. The condition is considered subacute when it has been present between 6 and 12 weeks. Chronic low back pain is often defined as pain persisting for more than 12 weeks.
The vast majority of patients with acute LBP can expect a favorable prognosis and a significant improvement within 6 weeks. However, recurrence rates are high and 5-20% of patients will go on to develop chronic LBP.
Contributing psychosocial factors, such as anxiety, depression, stress, and work dissatisfaction, may perpetuate the pain experience.
Definitive causes of LBP include disc herniation with suspected radiculopathy or spinal stenosis, osteoporotic compression fracture, inflammatory arthropathies, cancer, infection, cauda equine, and visceral pathologies such as aortic aneurysm, pelvic, gastrointestinal, and renal pathology. These definitive causes are uncommon, and the vast majority of patients presenting with back pain will have nonspecific LBP of a less clearly understood origin.
An estimated 80-90% of all back pain is nonspecific and caused by neuro-musculoskeletal dysfunctions emanating from ligament, facet joints, muscle, fascia, nerve roots, the vertebral periosteum or the outer portion of the disk.
A thorough history and physical exam can guide patients with acute and chronic low back pain. It is helpful to think in terms of three basic diagnostic categories: nonspecific LBP, back pain with suspected radiculopathy or spinal stenosis, or back pain that is a result of a specific pathology.
In most cases, imaging does not add useful information or value, can be harmful, and findings most commonly do not correlate to the clinical course of LBP. Without red flag symptoms or concerning neurological findings, imaging prior to 6 weeks of symptoms should be discouraged.
Integrative Therapy
Nutrition, exercise, and ergonomic awareness are important behaviors that may contribute to or perpetuate back pain. Additionally, biomechanical interventions include exercise therapy, spinal manipulation, non-thrust manual therapy such as muscle energy, strain-counterstrain, myofascial release, trigger point therapy, massage, and acupressure all reduce LBP symptoms.
Yoga and tai chi are also beneficial for chronic LBP, as are acetaminophen, NSAIDs, muscle relaxants, and opioids. Devil’s claw, Willow bark, topical analgesic cream, and CBD oil are superior to placebo
Over 4,000 research papers published showing effectiveness of acupuncture for pain including LBP. Epidural injection is effective for those with radicular symptoms and surgical interventions effective for patients with radicular symptoms and concordant herniated disk on imaging and those with severe neurogenic claudication from spinal stenosis.
Acupuncture
- Local points: BL23-34, 47, 50, 53, 54, GV 2-4, Ashi points.
- Distal points: BL 10, 40, 57, 60, KD 3, GV26.
- Add electric stimulation with low frequency for chronic LBP. One of the advantages of electro-acupuncture in the clinical practice is its ability to objectively and quantifiably define stimulus frequency and intensity which can optimize the effects of the traditional technique. Points used for electro-acupuncture: UB 22 (1.5cm lateral to L1 vertebrae), UB 26 (1.5cm lateral to L5), UB 50 (3cm lateral to T12), and UB 53 (3cm lateral to S2 vertebrae).
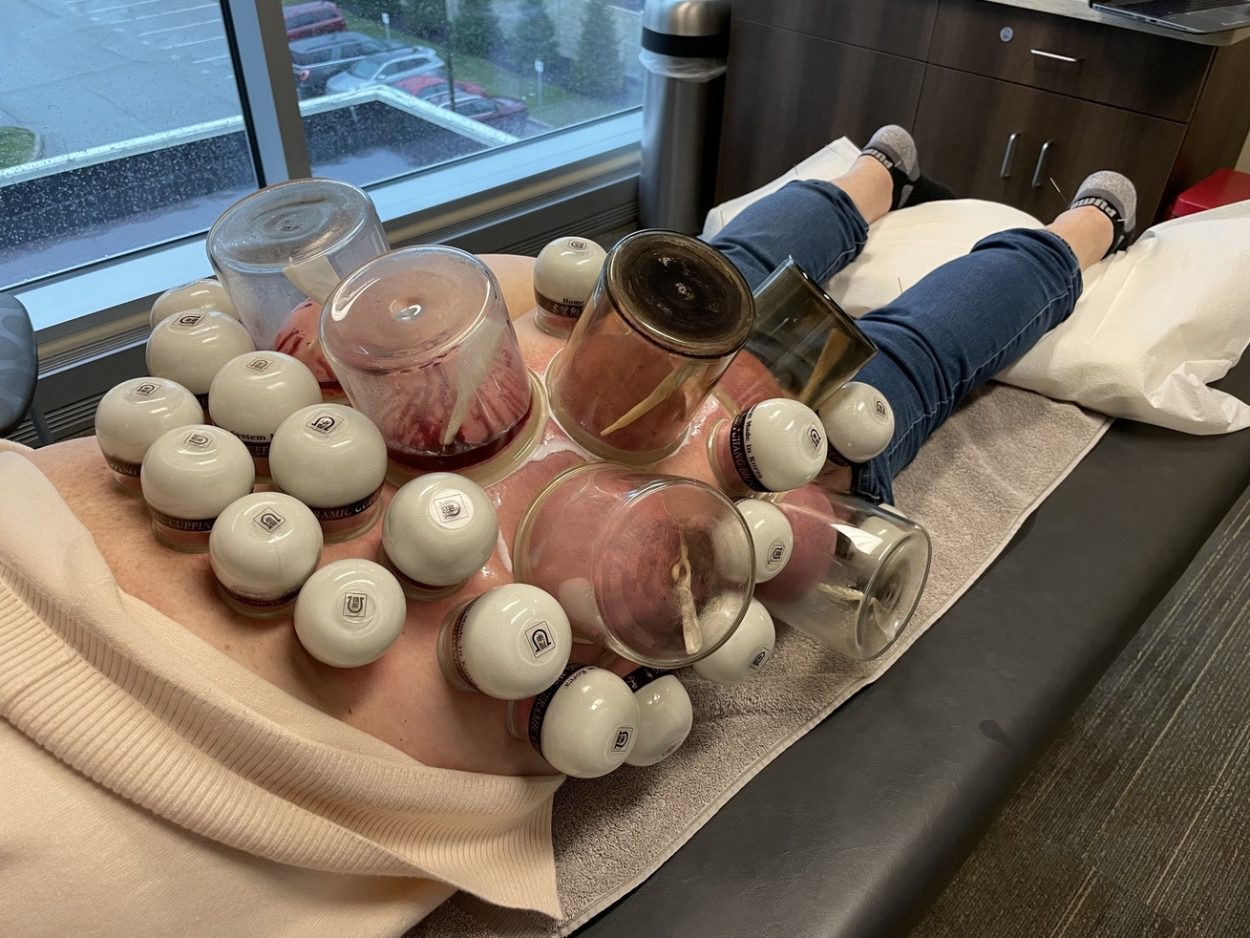
Cupping Therapy
- Both wet and dry cupping are effective for acute and chronic low back disorders.
- Cupping therapy is less effective for spinal stenosis, herniated disc, and sciatica.
- Use large cups of at least 4-inch diameter on the back.
- Apply small and medium size cups just above and below the affected area.
- Treat bilaterally for counterirritant effects.
- Cupping intensity: medium to strong
- Cupping method: local cupping and regional cupping
- Patients with radiculopathy: wet cupping lumbosacral area, BL40, 57, and lateral and posterior aspect of leg.
- Frequency of visit: once a week for 2 to 3 visits acute LBP and once every 2-4 weeks for chronic LBP.
- Placement of cupping, intensity of cupping, and frequency of cupping can vary depending on the location, the patient’s pain tolerance, and the underlying etiology of LBP.